In India, the role of trauma care systems becomes particularly important from the perspective of road safety given the consistently high number of road traffic fatalities and injuries for many decades now. Under Ministry of Health and Family Welfare’s Trauma Care Programme, concerted efforts are underway to “to bring down preventable deaths due to road accidents to 10 per cent by developing a pan-India trauma care network in which no trauma victim has to be transported for more than 50 kilometers and a designated trauma center is available at every 100 Km” (MoHFW, 2015). According to official records, a network of 196 trauma care facilities are available across the length and breadth of the country. With 11% of global road fatalities occurring in India, the network will have to grow denser and develop deep capabilities for specialized trauma care to reduce fatalities. Actions taken in the time between when a road crash occurs and the injured arrive at a hospital or trauma care center largely determine the likelihood of survival of the injured. However severe the injury may be, the bystander or the first responder available through the emergency number service (108 in India) must act swiftly to connect the injured with medical care and save precious minutes in this time interval. In the gradually evolving infrastructure of trauma systems in India, many links in the “trauma chain” (Fig 1) need to be strengthened to reduce morbidity and save lives affected during road crashes. Given the spatial distribution of road crashes in our country, often the onus of transferring the injured to the nearest hospital or trauma care facility relies on the courage and conscience of bystanders who happen to be around. It is this first link in the chain, “Bystander first aid”, that we have focused on through our intervention in Nagpur. And we like to call them ‘Trystanders’, since they ‘try’ to save lives out of a sense of responsibility and take action.
https://main.mohfw.gov.in/sites/default/files/Prog%20brief%20Trauma%20component%20.pdf
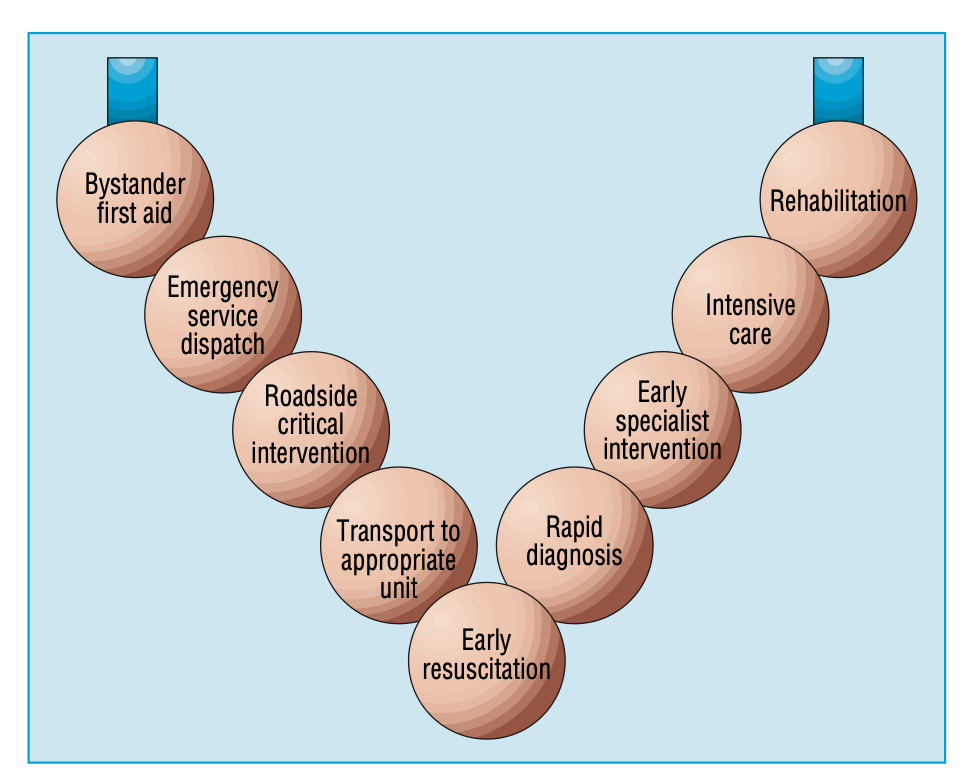
Source: Coats & Davies, BMJ 2002.
With the support of RoadMarc Foundation on our ongoing iRASTE project, we have gone a step further. With the blackspots identified on the basis of historical crash data, we have set up first aid kiosks at 8 locations in the Nagpur metropolitan region. To utilize these resources, we have created a community of first responders at each location by engaging with the local communities — shopkeepers, autorickshaw drivers, small vendors, auto repair shop workers, mechanics, other local people — who are anchored in these neighborhoods for their sources of livelihood. Our project members immersed themselves in these settings to propagate the message and essence of the intervention and ran a campaign to invite interest from the people. The community members who showed willingness to volunteer and take action in this public cause were registered to form a first responder team – Trystander cell — and the group pledged to take action to the best of their abilities in case s/he witnesses a crash in the vicinity of the kiosk. For the physical installation, a first aid box containing materials such as a foldable stretcher, different kinds of bandages, dettol, cloth materials, ointments, electral, etc. have been stored under lock and key – and each member has an individual key. The cell numbers of the team members have been painted on the panel of the kiosk along with messages to reinforce the role of human errors — like wrong side driving, not wearing helmets, violating traffic rules and more. The program has received great support and apppreciation from Nagpur City Police and Public Health Engineering department of the Nagpur Municipal Corporation. Within 3 months of the launch of these kiosks, the local teams were able to attend to atleast 10 road crash victims who suffered mild injuries.

Fig 2. Locations of Trystander Cells

Fig 3. Trystander team at Chinchbhavan Intersection. Dec 2023.
In the subsequent phase, the project team has planned to pour energies into developing clear protocols to communicate with the network of hospitals and trauma care centers in the region so that time it takes to transfer to the facility for definitive care is reduced in case of grievous injury. Decisions to spatially distribute trauma care systems must account for crash locations and the network of hospitals with specialized capabilities to reduce transport time of critically injured crash victims. Our endeavor to mobilize local communities for effective trystander first aid has sown the seed to support the larger efforts underway to save precious lives that get affected during travel on Indian roads and highways. Of course, we have to cover a long distance, and we are confident this is a solid first step in the right direction.